
Case-Report | DOI: https://doi.org/10.31579/2578-8868/104
*Corresponding Author: Amal Alqassmi, pediatric neurology at king Saud medical city
Citation: Alqassmi. A, Abdurhman A. (2020) Rare Variant in LAMA2 gene Causing Congenital Muscular Dystrophy. A Case Report. J. Neuroscience and Neurological Surgery. 6(2); DOI:10.31579/2578-8868/104
Copyright: © 2020 Amal AlQassmi, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 27 November 2019 | Accepted: 26 December 2019 | Published: 02 January 2020
Keywords: congenital muscular dystrophy; biochemistry; LAMA2 gene
The aim of this study was to characterize the clinical and genetic features of a 1-year-old female with merosin-deficient congenital muscular dystrophy type 1A (MDC1A). MDC1A is the most common form of congenital muscular dystrophy. MDC1A is caused by mutation of the laminin α-2 gene (LAMA2), localized to chromosome 6q22-23. Clinical presentation, as well as the results of neuroimaging, electrophysiology and molecular genetic tests were used to evaluate a patient with MDC1A. The patient presented with severe hypotonia and proximal weakness at 5.5 months of age, as well as delayed developmental milestones. The serum creatine kinase levels of the patient were elevated at 1620 IU/l. Magnetic resonance imaging (MRI) showed that the white matter in the frontal, parietal, temporal and occipital lobes was abnormal with low signal intensities on T1-weighted images and high signal intensities on T2-weighted images; the rest of study was normal. Sequencing of the 65 exons of the LAMA2 revealed a homozygous nonsense mutation in exon 50: a Ala>L exchange in nucleotide c.1762 that resulted in a stop codon (Ala588Leufs11 stop). Molecular genetic testing is a reliable method for confirming a diagnosis of MDC1A. When a patient presents with severe congenital hypotonia, muscle weakness, high serum creatine kinase (CK) levels and white matter abnormalities, the evaluation may directly proceed to molecular genetic testing of the LAMA2 gene.
Congenital muscular dystrophy type 1A (MDC1A) belongs to a group of neuromuscular disorders that beings at birth or infancy and is characterized mainly by hypotonia, muscle weakness and muscle wasting [1]. Other signs and symptoms include rigidity of the spine; scoliosis; and delayed, limited motor development. Respiratory problems, feeding disorders and seizures may also occur. With time, affected individuals may develop an elongated face and ophthalmoplegia disorders (paralysis or weakness in muscles of the eye). Intellectual development is typically normal. Merosin-deficient congenital muscular dystrophy type 1A (MDC1A) it is an autosomal recessive neuromuscular disorder caused by mutations in the laminin α-2 gene (LAMA2) on chromosome 6q22–23 that results in a deficiency of the laminin α-2 chain, a component of skeletal muscle extracellular matrix laminin-2, merosin [2]. In Saudi Arabia, MDC1A is an extremely rare condition with only few reported cases to date [3]. Patients with MDC1A have severe muscular weakness and atrophy, diffuse contractures, inability to walk and facial dysmorphism. In addition, they have markedly increased serum creatine kinase (CK) levels and have characteristic white matter abnormalities on cranial magnetic resonance imaging (MRI). With more widespread use of molecular genetic testing, these tests are becoming more important for confirming the diagnosis of CMD subtypes than are muscle biopsies. In the current study, we report a case of a young female with MDC1A whose diagnosis was confirmed by clinical presentation, characteristic white matter abnormalities and molecular genetic testing without the need for a muscle biopsy.
Case report
Clinical presentation
The 1.8 -year-old patient was the first daughter of a first degree consanguineous, healthy parents. The patient first admitted to Pediatrics intensive care unit at King Saud Medical City in Riyadh, at the age of 7 months due to respiratory distress and chest infection, patient had apnea and respiratory failure with Pco2 retention was intubated and treated and pneumonia covered by antibiotic and septic work up done wasnegative. Patient kept on ventilator for >2 weeks, neurology was consulted due to sever hypotonia and difficulty in extubating, every time they tried she will had apnea and pco2 retention. Developmental milestones were delayed at 6 months of age and the patient exhibited severe axial and peripheral hypotonia with feeding difficulties.
By 1 years of age, the patient was able to hold her head up, but was unable to roll over or sit alone. At the age of 1.5 years, the patient was able to sit supported, but not able to stand. Start to vocalize. The patient was born at 39 weeks of gestation and the birth weight was 2,800 g. The pregnancy and delivery were uneventful. A family history revealed no other cases of neuromuscular diseases. The study was approved by the Ethics Committee of King Saud medical city. Informed consent was obtained from the patients’ family.
When the patient was admitted as aspiration pneumonia at age of 7 months, ventilated started on antibiotic, was floppy and had difficulty to extubate, neurology was consulted the serum CK level was 1620 mU/ml and MRI revealed diffuse white matter dysplasia and the suspected diagnosis was adrenoleukodystrophy. On physical examination, the patient’s chest and abdomen were normal, as were the results of cardiac assessment. However, the patient exhibited severe axial hypotonia with bilateral upper and lower extremity weakness, which was more proximal than distal and predominantly at the shoulder and pelvic girdle, minimal limb movement The upper and lower limb proximal muscle strength was determined to be grade 3/5.The cranial nerves were normal and the patient had no difficulties on sensory examination and coordination. Deep tendon reflexes and Babinski’s sign were negative.
Laboratory test results were as follows: leukocyte count, 500 cells/μl; hemoglobin, 11.5 g/dl; hematocrit, 33.5%; and platelet count, 251×103 cells/μl.
Biochemistry test results
were as follows: glutamic oxaloacetic transaminase, 10 IU/l; glutamate alanine aminotransferase, 39 IU/l; CK, 1620 IU/l; CK-MB, 74 IU/l; triglycerides, 0.88 mmol/l; and ammonia, 10.0 μmol/l. Urine and blood screens for hereditary metabolic diseases were unremarkable Neuroimaging - Magnetic resonance imaging (MRI) results at 1 years of age. (A) Axial T2-weighted image and (C) coronal T2-weighted fluid attenuated inversion recovery (FLAIR) image show diffuse, symmetrical high signal intensities in the cerebral white matter. (B,) Axial T2-weighted image shows diffuse low signal intensity in the cerebral white matter magnetic resonance spectroscopy (MRS) was normal.
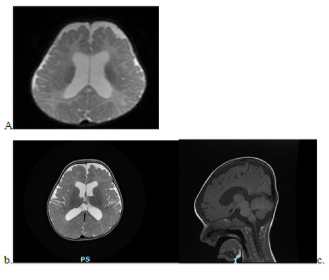
Figure 1: Magnetic resonance imaging (MRI) results at 1 years of age. (A) Axial T2-weighted image and (C) coronal T2-weighted fluid attenuated inversion recovery (FLAIR) image show diffuse, symmetrical high signal intensities in the cerebral white matter. (B,D) Axial T2-weighted image shows diffuse low signal intensity in the cerebral white matter
Electrophysiological studies
Electromyography (EMG) was used to aid in differentiating whether the patient’s deficits were myogenic or neurogenic. Needle EMG of the left and right tibia is anterior muscle suggested a myopathic process with reduced recruitment potential, decreased amplitude and duration of response, appearance of variable small amplitudes and short-duration polyphasic myogenic waves. Nerve conduction studies (NCS) were performed for the left tibial and left deep peroneal nerves using conventional methods. These revealed a normal motor nerve conduction velocity (MCV).
Molecular Genetic Testing
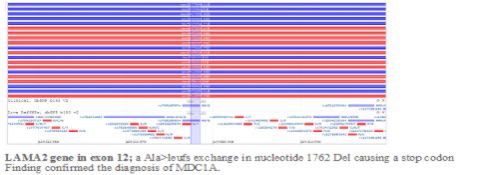
The patient in the present case was suspected of having MDC1A based on congenital hypotonia, delayed motor milestones and brain white matter abnormalities on MRI. Thus, molecular genetic testing was performed without a muscle biopsy. Genomic DNA from the patient and the patient’s parents was extracted from peripheral blood leukocytes using standard procedures. PCR and DNA direct sequencing were used to analyze all 65 exons of LAMA2 to determine if there were any gene mutations. DNA analysis revealed that the patient had a homozygous nonsense mutation in the LAMA2 gene in exon 12; a Ala>leufs exchange in nucleotide 1762 Del causing a stop codon
(Ala 588Leufs 11). The patient’s parents were heterozygotes for this mutation. This finding confirmed the diagnosis of MDC1A.
Discussion
MDC1A is caused by mutations in the LAMA2 gene and was first described by Tome et alin 1994 [2]. The estimated prevalence of CMDs is ~1 in 7 million [5]. In Europe, MDC1A accounts for ~40% of CMD cases [6]. MDC1A is characterized by congenital muscle hypotonia, delayed or arrested motor milestones and feeding difficulties. Muscle weakness is absent or slowly progressive and is accompanied by contractures that mostly affect the elbows, hips, knees and ankles. The majority of patients may achieve unsupported sitting; however, <10% achieve ambulation [7]. The common lifethreatening complications of MDC1A include respiratory failure and feeding difficulties. The patient in the present study was only 1.5 years old and had not suffered from any severe respiratory infections. However, with this disease, pulmonary infection is the most common cause of mortality, which may occur during the first decade or anytime thereafter. Treatment with non-invasive ventilation and tracheostomy may greatly improve health. In CMDs, the serum levels of CK are mildly to markedly elevated. In general, CMD subtypes with primary or secondary merosin deficiency, including dystroglycanopathies, show high serum CK concentrations, while those with no merosin deficiency show normal or mildly increased serum CK concentrations [8]. In the present case, the serum CK level was elevated to 1620 IU/l, which indicated primary or secondary merosin deficiency. EMG and NCS are recommended for all patients with suspected CMDs to confirm myopathy and to exclude other diseases. In the present case, EMG confirmed a myopathic process with early recruitment and decreased amplitude and duration of response, while the results of NCS were normal. In a number of cases of MDC1A, mild neuropathic changes may be observed since laminin α-2 is absent in the basement membranes surrounding Schwann cells and myelin sheaths [9]. The majority of patients with MDC1A have normal intellectual and speech development, although cases of learning disabilities and mental retardation have been reported [10]. Epilepsy has been estimated to occur in ~6–8% of these cases; seizures are partial and complex, with no consistent pattern [10]. In the present case, an EEG was normal; however, it is essential that a standard EEG is performed periodically for MDC1A patients.
Despite a minority that has clinical central nervous system findings, a consistent finding common to all patients >6 months of age is the presence of cerebral white matter abnormalities on neuroimaging. In the present case, cranial MRI revealed signal abnormalities in the white matter of the frontal, parietal, temporal and occipital lobes, whereas the cortex was normal. Children may initially be misdiagnosed as having a leukodystrophy. White matter changes do not regress with time. Although the pathophysiology of the white matter changes has not been completely elucidated, the majority of investigators postulate that disruption of the blood-brain barrier associated with laminin α-2 leads to increased water content, which results in abnormal white matter signal intensity [11,12]. The pattern of white matter abnormalities associated with MDC1A is characteristic as compared with other CMD subtypes. A small number of patients have structural changes with mild ventricular enlargement, focal cortical dysplasia, occipital polymicrogyria and hypoplasia of the pons and cerebellum [13]. Previously, a diagnosis of MDC1A was based on the clinical findings of severe congenital hypotonia, weakness associated with high CK blood levels, white matter abnormalities and dystrophy associated with negative immunostaining of biopsied muscle for merosin [14]. A muscle biopsy appears to be an essential factor in the diagnosis of MDC1A. However, with the more widespread use of molecular genetic testing for confirming the diagnosis of a CMD subtype, the recent trend has been to perform molecular genetic testing without a muscle biopsy when the medical history, physical examination and neurological examination support the diagnosis of a CMD.
In the present case, due to the congenital hypotonia, delayed motor milestones, markedly elevated CK concentration and brain white matter abnormalities on MRI, the patient was suspected of having MDC1A. Thus, we directly proceeded to molecular genetic testing without performing a muscle biopsy. Ultimately, a nonsense mutation in the LAMA2 gene confirmed our diagnosis of MDC1A.
This gene comprises 65 exons that encode for the α2 chain subunit of laminin-2. Laminin-2 is a heterotrimer consisting of laminin α-2, β-1 and γ-1 subunits [16]. Mutations in LAMA2 include nonsense, missense, deletion and splice-site mutations, which all result in a primary deficiency in the laminin α-2 chain of merosin [15,17]. Thus, for MDC1A, an evaluation may proceed directly to molecular genetic testing without a biopsy, depending on a typical presentation and following exclusion of other more common diagnoses. By contrast, if multiple genes need to be tested, such as for confirming a diagnosis of a dystroglycanopathy, the immunohistochemical analysis of a muscle biopsy may identify the subtype prior to molecular genetic testing.
MDC1A is the most common form of CMD. MDC1A is caused by a mutation of LAMA2 located on human chromosome 6q22–23. The typical presentations of MDC1A are severe congenital hypotonia, muscle weakness, elevated serum levels of CK and white matter abnormalities. To confirm a diagnosis of MDC1A, the evaluation may proceed directly to LAMA2 molecular genetic testing without the need for a muscle biopsy
Abbreviations:
CMDs congenital muscular dystrophies;
MDC1A merosin-deficient congenital muscular dystrophy type 1A;
MRI magnetic resonance imaging;
CK creatine kinase;
CK-MB creatine kinase-MB;
MRS magnetic resonance spectroscopy;
EMG electromyography;
NCS nerve conduction studies;
MCV motor nerve conduction velocity;
LAMA2 laminin α-2 gene
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
